La
enfermedad periodontal es una infección bacteriana de las encías que destruye
las fibras de incersión de la placa dental y el hueso de soporte que mantiene
los dientes en la boca. La principal causa de esta enfermedad es la placa
bacteriana, una película pegajosa, incolora que se forma constantemente en los
dientes. Las toxinas producidas por la bacteria en la placa inflaman las encías,
provocando la infección. El estado menos severo se conoce como gingivitis,
conforme avanza la enfermedad se forman bolsas estas se llenan de infección y
destruye mas tejido, hueso y los dientes eventualmente se aflojan y se pierden.
¿Cuáles son los síntomas de la enfermedad periodontal?
•
Sangrado al cepillarse o al usar el hilo dental.
• Encías que van dejan al descubierto las raíces de los dientes.
• Encías enrojecidas, agrandadas y fácilmente móviles.
• Dientes móviles y que se empiezan a separar.
• Pus entre la encía y el diente.
• Mal aliento persistente.
• Cambios en la posición de la mordida de los dientes.
• Cambios en los ajustes de las prótesis removibles.
• El incremento de espacio entre los dientes.
Sin
embargo es posible tener la enfermedad periodontal sin notar ninguno de estos
signos, por está razón es importante solicitar una evaluación periodontal.
¿Qué otros factores contribuyen a la enfermedad periodontal?
Diabetes.
Las enfermedades periodontales pueden ser más severas en diabéticos
no controlados. Enfermedades sistémicas.
La enfermedades que interfieren con el sistema inmunológico del cuerpo
pueden empeorar la condición de las encías. Embarazo y pubertad.
Algunos cambios hormonales pueden provocar que las encías se tornen rojas,
blandas y sangren fácilmente. Estrés.
Puede ocasionar que al cuerpo se le dificulte combatir una infección,
incluyendo las periodontales. Medicamentos.
Algunas drogas como los anticonceptivos orales, antidepresivos y
ciertos medicamentos para el corazón. Apretamiento ó rechinamiento de los dientes.
Esos hábitos pueden ejercer mucha presión en el tejido de soporte de los
dientes y acelerar la destrucción de los tejidos. Fumar.
Las personas que usan tabaco crean mayores posibilidades de adquirir
enfermedades periodontales. Mala alimentación.
Una dieta baja en nutrientes provoca que el cuerpo tenga dificultades de
combatir infecciones.
¿Cuál es el tratamiento para la enfermedad de las encías?
En las
etapas iniciales de la enfermedad de las encías, el tratamiento consiste en
remover la placa y cálculos de las bolsas alrededor de los dientes puliendo y
alisando las raíces. Así se eliminan las bacterias y los irritantes que causan
la inflamación.
Normalmente el tratamiento permite que la encía se adhiera de nuevo al diente o
se contraiga lo suficiente para eliminar la bolsa. En la mayoría de los casos de
la enfermedad periodontal inicial requiere un raspado, alisado radicular y una
buena higiene oral para obtener resultados satisfactorios.
¿Los casos más avanzados pueden requerir tratamiento quirúrgico?
En
casos todavía más avanzados donde pueden existir dientes flojos, se tratara
ajustando la mordida, por ejemplo, uniendo los dientes con férulas temporales
para reducir el movimiento obteniendo más comodidad y mejor función. Los
tratamientos adicionales pueden incluir Ortodoncia o la colocación de aparatos
protésicos.
¿Quien hace el tratamiento periodontal?
Los
periodoncistas tienen entrenamiento extenso y avanzado para tratar la enfermedad
periodontal, deben prepararse académicamente mínimo dos años después de haberse
graduado como odontólogos. Como especialistas dedican su tiempo, energía y
habilidades para atender a la gente que necesita el tratamiento de las encías.
La Periodoncia es una de las ocho especialidades reconocidas por la Asociación
Dental Americana (ADA).
¿Cómo puede prevenirse la enfermedad periodontal?
La
visitas regulares al dentista, la limpieza diaria mantendrá el sarro a un
mínimo, sin embargo no lo prevendrá totalmente. La limpieza profesional, por lo
menos dos veces al año es necesaria.
Consulte a un especialista, el le mostrará la manera de tener un cuidado con sus
dientes y una mejor salud dental por medio del hábito del cepillado y la
utilización del hilo dental.
Muchas personas no se dan cuenta cuán común son
las enfermedades periodontales (alrededor del diente) que comienzan lesionando
las encías. Tres (3) de cuatro (4) adultos poseen algún tipo de esta enfermedad.
En la mayoría de los casos, no produce dolor y por consiguiente, dicho problema
pasa desapercibido. Sin embargo, su temprana detección y tratamiento son
extremadamente importantes, debido a que la enfermedad periodontal termina con
la vida del diente (movilidad, infección, extracción).
Estos pequeños comentarios dan algunas respuestas a las preguntas más comunes
sobre esta enfermedad y pueden servirle de guía para obtener una buena salud
periodontal. Recordamos a Ud., que es una enfermedad crónica,
que su profesional tratará de frenar la evolución para
salvarle sus piezas dentales y que éstas permanezcan el mayor tiempo posible en
su boca. Sus dientes son más valiosos que cualquier reemplazo que su Odontólogo
pueda ofrecerle.
¿De qué se trata?.. piorrea, paradentosis, periodoncia, movilidad dental,
periodontítis, etc.. Los problemas en las encías son infecciones provocadas por
una película de bacterias (“placa dental”), que se
adhiere a la superficie dental justo en el límite con las encías. Puede ocurrir
a cualquier edad, pero por lo general es frecuente después de los 40 años de
edad. En los primeros estadíos de la enfermedad, denominada gingivitis, las
encías se tornan rojizas y sangran con facilidad. A medida que avanza la
infección hacia el hueso que soporta a los dientes, recibe el nombre de
periodontítis, y en este momento puede provocar un daño irreversible. Cuando
avanza más todavía, el hueso y los tejidos que soportan al diente son destruidos
provocando la caída o la extracción dental.
¿Qué provoca los problemas?..: son provocados por las bacterias que se adhieren
en forma de película, organizándose en la llamada “placa dental”.
Es pegajosa y se forma constantemente; en caso de no remover esta placa en forma
diaria con el cepillado, libera toxinas que irritan, inflaman e infectan a la
encía. Más adelante estas toxinas destruyen la encía y provocan que los tejidos
se separen del diente y formen un espacio profundo: “bolsas”.
Estas bolsas, de hecho acumulan más bacterias dando lugar a un círculo vicioso
que agrava la situación, migrando hacia la raíz del diente y dándole apariencia
de dientes mucho mas grandes, cuando lo que sucede es que el hueso se reabsorbe
y desciende (o asciende en dientes sup.) la encía.
Diente sano
Gingivitis
Periodontitis
Infeccion
de las encias
La
Periodoncia es una rama de la Odontología que se encarga del estudio
y tratamiento de los tejidos que rodean y dan soporte a los dientes;
Existen múltiples alteraciones que pueden afectar a estos tejidos,
entre los más comunes está la gingivitis (inflamación crónica de las
encías), y la periodontitis (pérdida parcial o total del hueso
soporte). Los tratamientos periodontales actuales utilizan un sin
número de nuevas técnicas y materiales que permiten conservar los
dientes por más tiempo y en mejores condiciones.
¿Es verdad
que con la edad esta uno predeterminado a perder sus dientes?
La principal causa responsable de la pérdida de dientes es la
enfermedad periodontal, esta produce una pérdida gradual del hueso
que soporta al diente, produciendo la caída de los mismos. Evitar
este padecimiento es tan fácil como mantener un adecuado control de
placa bacteriana y acudir regularmente con el dentista. Recuerde que
un buen cuidado de su boca le permite mantener los dientes para toda
su vida.
Un adecuado tratamiento parodontal a tiempo evita
la perdida de hueso de soporte y encía.
¿Cómo se tratan los padecimientos de las encías?
Actualmente existen una gran variedad de innovadoras técnicas y
materiales en periodoncia que permiten controlar y mejorar las
condiciones de las encías y del hueso de soporte. Injertos óseos y
gingivales así como una gran variedad de técnicas facilitan y
mejoran considerablemente el pronóstico de estos padecimientos.
Antes
Después
Injertos óseos
y gingivales se realizan en algunas ocasiones para preservar las
estructuras de soporte de los dientes o para impedir la pérdida
severa de hueso en la zona de extracción de una pieza dental, lo que
permite sustituir al diente perdido de una mejor y más fácil manera.
Tratamiento periodontal con LASER:
Antes/Before Despues/After
Thanks to
its bactericidal effect the laser can quickly and thoroughly
decontaminate gingival pockets: this produces a significant
reduction of bacteria and avoids a long and uncomfortable
recovery. Through the natural analgesic and biostimulating
effects of laser irradiation, patients usually have minimal
post-operative discomfort. The diode laser is useful for the
treatment of:
Laser soft tissue curettage
Laser removal of diseased,
infected, inflamed, and necrosed soft tissue within the
periodontal pocket
Removal of highly inflamed
edematous tissue affected by bacteria penetration of the
pocket lining and junctional epithelium
Sulcular debridement (removal of
diseased or inflamed soft tissue in the periodontal
pocket to improve clinical indices including: gingival
index, gingival bleeding index, probe depth, attachment
loss and tooth mobility).
Periodontal
Disease
Highlights
Symptoms of
Periodontal Disease
Symptoms of
periodontal disease
include red and
swollen gums,
persistent bad
breath, and gum
recession and loose
teeth. Smoking,
certain types of
illnesses
(diabetes), older
age, and other
factors increase the
risk for periodontal
disease. If you have
periodontal disease,
your dentist may
refer you to a
periodontist, a
dentist who
specializes in
treating this
condition.
Practice Good Dental
Hygiene
Consistent good
dental hygiene can
help prevent
gingivitis and
periodontitis. The
American Dental
Association
recommends that
everyone:
Brush twice
daily with a
fluoride
toothpaste (be
sure to replace
toothbrushes
every 3 - 4
months).
Clean between
the teeth with
floss or an
interdental
cleaner.
Eat a well-balanced
diet and limit
between meal
snacks.
Have regular
visits with a
dentist for
teeth cleaning
and oral
examinations.
Mouthwashes
According to the
American Dental
Association,
antimicrobial
mouthwashes may
provide additional
oral health benefits
for preventing and
reducing gingivitis
and plaque. However,
they are not a
substitute for daily
brushing and
flossing.
Complications
Uncontrolled
periodontal disease
is associated with:
Tooth loss
Bad breath
Heart problems
such as heart
disease and
stroke
Diabetes
Respiratory
diseases
Premature
delivery and low
birth weight
Introduction
Periodontal disease
refers to a group of
problems that arise
in the sulcus, the
gap between the gum
and the tooth.
What
is the Periodontium?
The part of the
mouth that consists
of the gum and
supporting
structures is called
the periodontium. It
is made up of the
following parts:
Gum (gingiva).
When healthy,
the gingiva is
pale pink, firm,
and does not
move. It has a
smooth or
speckled texture.
The gingival
tissue between
teeth is shaped
like a wedge.
The space
between the gum
and tooth,
called the
sulcus
Root surface (the
cementum)
Connective
tissue
Bone. The crest
of the
supporting bone,
which can be
viewed on x-rays,
is normally 2 mm
below the point
where the crown
of the tooth
meets the root (the
cementoenamel
junction).
The
structure
of the
tooth
includes
dentin,
pulp and
other
tissues,
blood
vessels,
and
nerves
imbedded
in the
bony jaw.
Above
the gum
line,
the
tooth is
protected
by the
hard
enamel
covering.
Periodontal Disease
Periodontal diseases
are generally
divided into two
groups:
Gingivitis,
which causes
lesions (wounds)
that affect the
gums
Periodontitis,
which damages
the bone and
connective
tissue that
supports the
teeth
The process starts
with bacteria. Even
in healthy mouths,
the sulcus is
teeming with
bacteria, but they
tend to be harmless
varieties.
Periodontal disease
develops usually
because of two
events in the oral
cavity: an increase
in bacteria quantity
and a change in
balance of bacterial
types from harmless
to disease-causing
bacteria. These
harmful bacteria
increase in mass and
thickness until they
form a film called
plaque.
In
healthy mouths,
plaque itself
actually provides
some barrier against
outside bacterial
invasion. When it
accumulates to
excessive levels,
however, plaque
sticks to the
surfaces of the
teeth and adjacent
gums and causes
cellular injury,
with subsequent
swelling, redness,
and heat.
When plaque is
allowed to remain in
the periodontal area,
it transforms into
calculus (commonly
known as tartar
). This material has
a rock-like
consistency and
grabs onto the tooth
surface. It is much
more difficult to
remove than plaque,
which is a soft mass.
The most important
component leading to
the disease process,
however, is the
body's persistent
immune response to
the bacterial
plaque. Specific
immune factors are
released that cause
inflammation and
damage that
eventually destroys
the support
structures and bone
and can lead to
tooth loss.
Gingivitis
Gingivitis is an
inflammation of the
gingiva, or gums. Is
nearly always
chronic, but an
acute form
infrequently occurs.
Chronic Gingivitis.
Ordinary chronic
gingivitis affects
over 90% of the
population. It is
characterized by
tender, red, swollen
gums that bleed
easily and may be
responsible for bad
breath (halitosis)
in some cases.
Treatment is very
effective if
initiated early in
the course of
gingivitis. Without
good management,
however, the problem
can progress.
Periodontitis
Periodontitis is
characterized by the
following:
Gum inflammation,
with redness and
bleeding
Deep pockets (greater
than 3 mm in
depth) that form
between the gum
and the tooth
Loose teeth,
caused by loss
of connective
tissue
structures and
bone
Gingivitis precedes
periodontitis,
although it doesn't
always lead to this
more severe
condition. In fact,
some research
suggests it is an
entirely different
disease. There are
different categories
of periodontal
disease, including:
Chronic
Periodontitis.
Chronic
periodontitis (also
referred to as adult
periodontitis) may
begin in adolescence
as a slowly
progressing disease
that becomes
clinically
significant in the
mid-30s and
continues throughout
life. Some dentists
question whether it
is a chronic,
unrelenting
condition and
instead suggest that
it waxes and wanes
depending on the
response of the
immune system.
Aggressive
Periodontitis.
Aggressive
periodontitis (also
referred to as early
onset periodontitis)
often occurs in
young people. It is
subdivided according
to whether it begins
before or after
puberty. Immune
deficiencies and a
genetic link have
been shown to be
possible factors for
all types of
aggressive
periodontitis. If
the condition is
localized and
treated, the outlook
is positive. People
with severe and
widespread
aggressive
periodontitis are at
high risk for tooth
loss.
Periodontitis
that occurs
before puberty
is very rare. It
begins with the
eruption of
primary teeth in
the first year
and causes
severe
inflammation and
bone and tooth
loss.
Juvenile
periodontitis
begins at
puberty and is
defined by
severe bone loss
around the first
molars and
incisors. It is
more common in
girls than in
boys. The
clinical signs
-- such as
inflammation,
bleeding, and
heavy plaque
accumulation --
are not present
in this
relatively rare
disease. The
treatment is the
same as in
chronic
periodontitis.
Rapidly
progressive
periodontitis
occurs in the
early 20s to mid-30s.
Severe
inflammation and
rapid bone and
connective
tissue loss
occur, and tooth
loss is possible
within a year of
onset.
Disease-Related
Periodontitis.
Periodontitis can
also be associated
with a number of
systemic diseases,
including type 1
diabetes, Down
syndrome, AIDS, and
several rare
disorders of white
blood cells.
Acute
Necrotizing
Periodontal Disease.
Acute necrotizing
periodontal disease
is an acute
infection in the
gums. It is
characterized by:
Black, dead
tissue
(necrosis)
Spontaneous
bleeding
Rapid onset of
pain
Bad odor
Blunted gum
tissue (tissue
is normally
cone-shaped)
Stress, poor diet,
smoking, and viral
infections are
predisposing factors
for this acute
necrotizing
periodontal disease.
Symptoms
In
general, symptoms
progress over time
and include:
Red and Swollen
Gums
Gum Bleeding.
Bleeding of the
gums, even
during brushing,
is a sign of
inflammation and
the major marker
of periodontal
disease. One
exception is
juvenile
periodontitis,
in which
symptoms are
mild or even
absent. It
should be noted
that the gums of
smokers with
periodontal
disease tend to
bleed less than
nonsmokers.
Bad Breath.
Debris and
bacteria can
cause a bad
taste in the
mouth and
persistent bad
breath.
Gum Recession
and Loose Teeth.
As the disease
advances the
gums recede, and
supporting
structure of
bone is lost.
Teeth loosen,
sometimes
causing a change
in the way the
upper and lower
teeth fit
together when
biting down or
how partial
dentures fit.
Abnormally
bulging,
protruding,
or
swollen
gums are
a
possible
sign of
disease.
Abscesses.
Deepening
periodontal
pockets between
the gums and
bone can become
blocked by
tartar or food
particles.
Infection-fighting
white blood
cells become
trapped and die.
Pus forms, and
an abscess
develops.
Abscesses can
destroy both gum
and tooth tissue,
cause nearby
teeth to become
loose and
painful, and may
cause fever and
swollen lymph
nodes.
Pain is usually not
a symptom, which
partly explains why
the disease may
become advanced
before treatment is
sought and why some
patients avoid
treatment even after
periodontitis is
diagnosed.
Causes
Periodontal disease
is marked by
bacterial overgrowth.
However, a
persistent immune
response to chronic
infections in the
mouth is believed to
play a major role in
gum destruction.
Bacterial Culprits
Reachers have found
more than 350
species of
microorganisms in
the typical healthy
mouth. Periodontal
infections are
linked to fewer than
5% of these species.
Healthy and disease-causing
bacteria can
generally be grouped
into two categories:
The harmless or
helpful bacteria
are usually
known as gram
positive aerobic
bacteria.
In periodontal
disease, the
bacterial
balance shifts
over to gram
negative
anaerobic
bacteria.
Inflammatory
disease and
injury cannot
develop without
these bacteria.
Following are some
of the bacteria most
implicated in
periodontal disease
and bone loss:
Actinobacillus
actinomycetemcomitans
and
Porphyromonas
gingivalis.
These two
bacteria appear
to be
particularly
likely to cause
aggressive
periodontal
disease. Both
P.
gingivalis
and A.
actinomycetemcomitans,
along with
multiple deep
pockets in the
gum, are
associated with
resistance to
standard
treatments for
gum disease.
P. gingivalis
may double the
risk for serious
gum disease.
P. gingivalis
produces enzymes,
such as one
called
arginine-specific
cysteine
proteinase, that
may disrupt the
immune system
and lead to
subsequent
periodontal
connective
tissue
destruction.
Bacteroides
forsythus
is also strongly
linked to
periodontal
disease.
Other bacteria
associated with
periodontal
disease are
Treponema
denticola, T.
socranskii,
and P.
intermedia.
These bacteria,
together with
P. gingivalis,
are frequently
present at the
same sites, and
are associated
with deep
periodontal
pockets.
Some bacteria are
related to
gingivitis, but not
plaque development.
They include various
streptococcal
species.
The
Autoimmune and
Inflammatory
Response
Evidence indicates
that periodontal
disease is an
autoimmune disorder,
in which immune
factors in the body
attack the person's
own cells and tissue
-- in this case,
those in the gum. It
appears to work like
this:
The bacteria
that form plaque
and tartar
release toxins
that stimulate
the immune
system to
overproduce
powerful
infection-fighting
factors called
cytokines.
Ordinarily,
cytokines are
important for
healing. In
excess, however,
they can cause
inflammation and
severe damage.
In addition,
white blood
cells produced
by the immune
response to
bacteria also
release a family
of enzymes
called matrix
metalloproteinases
(MMPs), which
break down
connective
tissue.
Studies suggest that
this inflammatory
response may have
damaging effects not
only in the gums but
also in organs
throughout the body,
including the heart.
Viral
Causes
Certain herpes
viruses (herpes
simplex and
varicella-zoster
virus, the cause of
chickenpox and
shingles) are known
causes of
gingivitis. Other
herpes viruses (cytomegalovirus
and Epstein-Barr)
may also play a role
in the onset or
progression of some
types of periodontal
disease, including
aggressive and
severe chronic
periodontal disease.
All herpes viruses
go through an active
phase followed by a
latent phase and
possibly
reactivation.
These viruses may
cause periodontal
disease in different
ways, including
release of tissue-destructive
cytokines,
overgrowth of
periodontal
bacteria,
suppressing immune
factors, and
initiation of other
disease processes
that lead to cell
death.
Risk Factors
More than 75% of
American adults have
some form of gum
disease, but
according to a major
survey, only 60%
have any significant
knowledge about the
problem. Gum
inflammation and
ulcers are common,
and not all people
with these problems
develop periodontal
disease. Still,
about 30% of people
are genetically
susceptible to
periodontal disease.
Other factors also
put individuals at
higher risk.
Oral
Environment
Lack
of Oral Hygiene.
Lack of oral hygiene
encourages bacterial
buildup and plaque
formation.
Sugar
and Acid.
The bacteria that
cause periodontal
disease thrive in
acidic environments.
Therefore, eating
sugars and other
foods that increase
the acidity in the
mouth increase
bacterial counts.
Poorly Contoured
Restorations.
Poorly contoured
restorations
(fillings or crowns)
that provide traps
for debris and
plaque can also
contribute to its
formation.
Anatomical Tooth
Abnormalities.
Abnormal tooth
structure can
increase the risk.
Wisdom Teeth.
Wisdom teeth, also
called third molars,
can be a major
breeding ground for
the bacteria that
cause periodontal
disease. In fact,
for patients in
their 20s,
periodontal disease
is most likely to
occur around the
wisdom teeth.
Periodontitis can
occur in wisdom
teeth that have
broken through the
gum as well as teeth
that are impacted
(buried).
Periodontal disease
can also be present
even in patients
with wisdom teeth
who do not have any
symptoms.
Adolescents and
young adults with
wisdom teeth should
have a dentist check
for signs of
periodontal disease.
Age
Children and
Adolescents.
Gingivitis, in
varying degrees, is
nearly a universal
finding in children
and adolescents. In
rare genetic cases,
children and
adolescents are
subject to
destructive forms of
the disease.
Researchers have
also observed some
of the organisms
seen in periodontal
disease in young
children without
signs of gum
problems. Healthy
children, however,
do not generally
harbor two primary
periodontal
bacteria, P.
gingivalis and
T. denticola.
The disease is also
uncommon in
teenagers.
Adults.
As people age, the
risk for periodontal
disease increases.
Over half of
American adults have
gingivitis
surrounding 3 - 4
teeth, and 30% have
significant
periodontal disease
surrounding 3 - 4
teeth. In a study of
people over 70 years
old, 86% had at
least moderate
periodontitis, and
over a quarter of
them had lost their
teeth.
Female Hormones
About three-quarters
of periodontal
office visits are
made by women, even
though women tend to
take better care of
their teeth than men.
Female hormones
affect the gums, and
women are
particularly
susceptible to
periodontal problems.
Hormone-influenced
gingivitis appears
in some adolescents,
in some pregnant
women, and is
occasionally a side
effect of birth
control medication.
Before Menstruation.
Gingivitis may flare
up in some women a
few days before they
menstruate, when
progesterone levels
are high. Gum
inflammation may
also occur during
ovulation.
Progesterone dilates
blood vessels
causing inflammation,
and blocks the
repair of collagen,
the structural
protein that
supports the gums.
Pregnancy.
Hormonal changes
during pregnancy can
aggravate existing
gingivitis, which
typically worsens
around the second
month and reaches a
peak in the eighth
month. Pregnancy
does not cause gum
disease, and simple
preventive oral
hygiene can help
maintain healthy
gums. Any pregnancy-related
gingivitis usually
resolves within a
few months of
delivery. Because
periodontal disease
can increase the
risk for low-weight
infants and cause
other complications,
it is important for
pregnant women to
see a dentist.
Oral
Contraceptives.
Some studies report
that oral
contraceptives
containing the
synthetic
progesterone
desogestrel (but not
dienogest, another
common progesterone)
increase the risk
for periodontal
disease.
Menopause.
Estrogen deficiency
after menopause
reduces bone mineral
density, which can
lead to bone loss.
Bone loss is
associated with both
periodontal disease
and osteoporosis.
Bone loss in the
alveolar bone (which
holds the tooth in
place) may be a
major predictor of
tooth loss in
postmenopausal
women. Periodontal
disease is the main
cause of alveolar
bone loss. During
menopause, some
women may also
develop a rare
condition called
menopausal
gingivostomatitis,
in which the gums
are dry, shiny, and
bleed easily. Women
may also experience
abnormal tastes and
sensations (such as
salty, spicy,
acidic, and burning)
in the mouth.
Family Factors
Periodontal disease
often occurs in
members of the same
family. Genetics,
intimacy, hygiene,
or a mixture of
factors may be
responsible. Studies
have found that
children of parents
with periodontitis
are 12 times more
likely to have the
bacteria thought to
be responsible for
causing plaque and,
eventually,
periodontal disease.
Genetic Factors.
Genetic factors may
play the critical
role in half the
cases of periodontal
disease. Up to 30%
of the population
may have some
genetic
susceptibility to
periodontal disease.
Intimacy.
Intimate partners
and spouses of
people with
periodontal disease
may also be at risk.
Researchers have
found that the
bacteria P.
gingivalis may
be contagious after
exposure to an
infected person over
a long period of
time. There is no
risk from short
exposure, such as
after a fast kiss or
when sharing an
eating utensil.
Smoking and Nicotine
Smoking is the
single major
preventable risk
factor for
periodontal disease.
The habit can cause
bone loss and gum
recession even in
the absence of
periodontal disease.
A number of studies
indicate that
smoking and nicotine
increase
inflammation by
reducing oxygen in
gum tissue and
triggering an over-production
of immune factors
called cytokines (specifically
ones called
interleukins). In
excess, cytokines
are harmful to cells
and tissue.
Furthermore, when
nicotine combines
with oral bacteria,
such as P.
gingivalis, the
effect produces even
greater levels of
cytokines and
eventually leads to
periodontal
connective tissue
breakdown. Smokers
may be more than 10
times more likely
than nonsmokers to
harbor the bacteria
that cause
periodontal disease
and are also more
likely to have
advanced periodontal
disease.
The risk of
periodontal disease
increases with the
number of cigarettes
smoked per day.
Smoking cigars and
pipes carries the
same risks as
smoking cigarettes.
Exposure to
secondhand smoke may
also be associated
with an increased
risk for developing
periodontal disease,
according to one
study. Fortunately,
when smokers quit,
their periodontal
health gradually
recovers to a state
comparable to that
of nonsmokers.
Some research also
indicates that
regular cannabis (marijuana)
smoking also
increases the risk
of periodontal
disease.
Diseases Associated
with Periodontal
Disease
Diabetes.
Much evidence exists
on the link between
type 1 and 2
diabetes and
periodontal disease.
Diabetes causes
changes in blood
vessels, and high
levels of specific
inflammatory
chemicals such as
interleukins, that
significantly
increase the chances
of periodontal
disease. High levels
of triglycerides (which
are common in type 2
diabetes) also
appear to impair
periodontal health.
Obesity, common in
people with type 2
diabetes, may also
predispose a person
to gum disease.
Controlling both
type 1 and 2
diabetes may help
reduce periodontal
problems. For
children with
diabetes, good oral
hygiene should begin
at a young age.
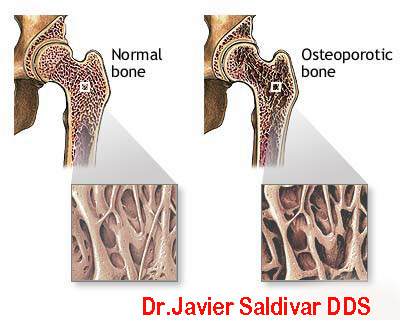
Osteoporosis and
Osteonecrosis.
Osteoporosis (loss
of bone density) has
been associated with
periodontal disease
in postmenopausal
women.
There have been a
few reports of
osteonecrosis (bone
decay) of the jaw in
patients who take
oral bisphosphonate
drugs such as
alendronate (Fosamax).
However, almost all
cases of
osteonecrosis of the
jaw associated with
bisphosphonate drugs
occur during or
after the use of
intravenous
bisphosphonates,
usually given as
part of treatment
for bone cancer or
other cancers that
have spread to the
bone. Symptoms of
osteonecrosis of the
jaw include loose
teeth, exposed
jawbone, pain or
swelling in the jaw,
gum infections, and
poor healing of the
gums.
Osteoporosis
is a
condition
marked
by
progressive
loss of
bone
density,
thinning
of bone
tissue,
and
increased
risk of
fractures.
Osteoporosis
may
result
from
disease,
dietary
or
hormonal
deficiency,
or
advanced
age.
Regular
exercise
and
vitamin
and
mineral
supplements
can
reduce
and may
even
reverse
loss of
bone
density.
As
a precaution, the
American Dental
Association (ADA)
recommends that
patients who are
prescribed or are to
receive
bisphosphonate drugs
get a thorough
dental exam before
beginning drug
therapy, or as soon
as possible after
beginning therapy.
The ADA also
recommends that
patients who take
oral bisphosphonate
drugs should discuss
with their dentists
any potential risks
from dental
procedures (such as
extractions and
implants) that
involve the jawbone.
In any case, be sure
to inform your
dentist if you are
taking a
bisphosphonate drug.
Your dentist or oral
surgeon may need to
take special
precautions when
performing dental
surgery.
Herpes-Related
Gingivitis.
Herpes virus is a
common cause of
gingivitis in
children and has
become increasingly
common in adults. It
typically starts out
with a purplish
color and "boggy"
sensation in the
gums. Multiple
blisters may form
across the mucus
membranes in the
mouth and gums,
followed by ulcers.
They usually resolve
in 7 - 14 days.
HIV-Associated
Gingivitis.
HIV-associated
gingivitis has been
reported in 15 - 50%
of patients with HIV
or AIDS.
HIV-positive
individuals harbor
larger numbers of
periodontal bacteria
(candida albicans,
P. gingivalis, black-pigmented
anaerobic rods, and
A.
actinomycetemcomitans)
than people without
HIV. Severe pain is
characteristic,
along with odor,
spontaneous bleeding,
ulcers, and swollen,
bright red gums. The
inflammation never
recedes, but
halitosis and acute
episodes can be
managed by
conventional
cleaning treatments.
Its severest form,
known as necrotizing
stomatitis, can be
diagnostic for AIDS.
In addition to
bleeding, the gums
in the front of the
mouth are a
yellowish-gray
color, and bone
thrusts out.
Autoimmune Diseases.
Autoimmune
conditions (Crohn's
disease, multiple
sclerosis,
rheumatoid arthritis,
lupus erythematosus,
CREST syndrome) have
been associated with
a higher incidence
of periodontal
disease. Some
research suggests
that periodontal
disease may even
play some causal
role. Still, more
research is needed
to determine a
definitive
association between
these diseases.
Other
Diseases.
People with
tuberculosis,
syphilis, Wegener's
granulomatosis,
amyloidosis, and
many genetic
disorders are also
at higher risk for
periodontitis.
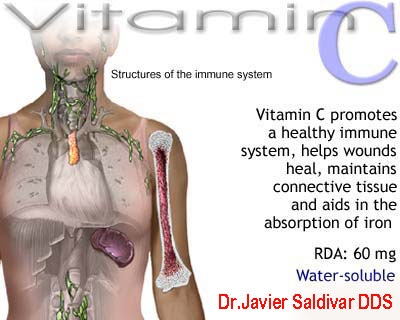
Vitamin C
Deficiencies
Vitamin C helps the
body repair and
maintain connective
tissue, and its
antioxidant effects
are important in the
presence of tissue-destroying
oxidants in
periodontal disease.
Research indicates
that vitamin C
deficiency
contributes to
periodontal disease.
Vitamin C levels are
especially depleted
in smokers. Eating
citrus fruits high
in vitamin C (such
as grapefruit) may
be helpful for
patients with
periodontitis.
Ethnic,
Socioeconomic, and
Geographic Factors
Dental disease is
most likely to
affect the poor.
Children and the
elderly suffer the
worst oral care, and
ethnic minorities
follow. In the
United States, the
lack of access to
dental insurance is
a contributing
factor.
Drug-Induced
Gingivitis
Gingival overgrowth
can be a side effect
of nearly 20
different drugs,
most commonly
phenytoin (Dilantin),
cyclosporine (Sandimmune),
and a short-acting
form of the calcium
channel blocker
nifedipine (Procardia).
Other
Causes of Gum
Inflammation
Several other
conditions can also
cause gum
inflammation, and
some have been
associated with
periodontal disease.
They include:
Mouth breathing
Psychologic
stress. Stress
can affect the
immune system.
Some studies
suggest that
stress can
influence the
development of
chronic
inflammatory
diseases, like
periodontitis.
Alcohol abuse.
One study
reported a
higher incidence
of periodontal
disease, tooth
decay, and
possibly
precancerous
areas in
patients who
abuse alcohol.
Canker sores (aphthous
ulcers)
Image of a
canker sore.
Self-injury in
psychologically
disturbed
patientsHereditary
gingival
fibromatosis. A
rare genetic
disease
associated with
both gum
overgrowth and
hairiness. It is
often associated
with gingivitis
and periodontal
disease.
Desquamative
gingivitis. With
this condition
the outer layer
of the gum
tissue
desquamates (peels
away), exposing
an acutely red
surface. It
usually occurs
as a result of
an allergic
reaction or of
skin diseases
such as lichen
planus, benign
mucous membrane
pemphigoid,
bullous
pemphigoid, and
pemphigus
vulgaris. This
condition
generally
resolves when
the underlying
problem is
treated. It is
fairly common in
middle-aged
women.
Complications
The ultimate outcome
of uncontrolled
periodontal disease
is tooth loss. As
the destructive
factors cause the
breakdown of bone
and connective
tissue, teeth lose
their anchor.
Bad
Breath
A
much less severe but
nevertheless
distressing problem
caused by
periodontal disease
is bad breath,
although coatings on
the tongue may
contribute more to
bad breath than
periodontal disease.
Heart
Disease and Stroke
Studies have
reported that people
who have heart
disease have a 1.5 -
4 times increased
risk for periodontal
disease. (The risk
is highest for
patients with
extensive gum
disease, bleeding
from every tooth.)
Acute coronary
syndrome, high blood
pressure (hypertension),
and high cholesterol
have also been
associated with
periodontal disease.
Periodontal disease
has also been linked
to stroke and
coronary artery
disease (CAD). The
more severe the
periodontitis, the
greater the risk for
heart problems.
However, it is still
not clear whether
periodontal disease
is a risk factor for
stroke or a marker
that reflects
various risk factors
common to both
conditions.
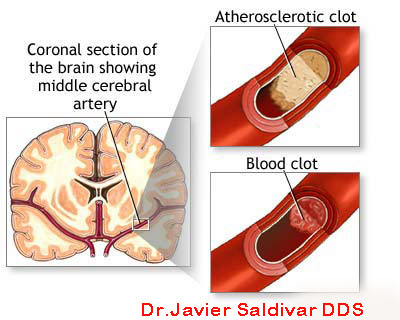
A stroke
is
caused
by a
loss of
blood
circulation
to areas
of the
brain.
The
blockage
usually
occurs
when a
clot or
piece of
atherosclerotic
plaque
breaks
away
from
another
area of
the body
and
lodges
within
the
blood
vessels
of the
brain.
An
inflammatory
response may be the
common element. This
is an over-reaction
of the immune system
that causes injury
to tissues in the
body. Patients with
heart conditions and
periodontal disease
may have elevated
levels of C-reactive
protein (CRP), which
indicates
inflammation is
present. Some
research indicates
that this
inflammatory
response can also
cause injury in the
arteries supplying
blood to the heart.
Other evidence
suggests that the
periodontal disease
bacteria themselves
-- particularly
P. gingivalis,
T. denticola,
T. forsythia,
and streptococci
species -- may be
associated with
thicker carotid
arteries (a
predictor of heart
attack and stroke),
regardless of
C-reactive protein
levels. It is still
not clear if
periodontal disease
actually causes
heart disease.
It
is also not clear if
treating gum disease
can reduce the risks
of heart disease and
improve health
outcomes for
patients with
periodontal disease
and vascular heart
problems. Studies
have been mixed, but
research is ongoing.
Effect on Diabetes
Diabetes is not only
a risk factor for
periodontal disease
-- periodontal
disease itself can
worsen diabetes and
make it more
difficult to control
blood sugar.
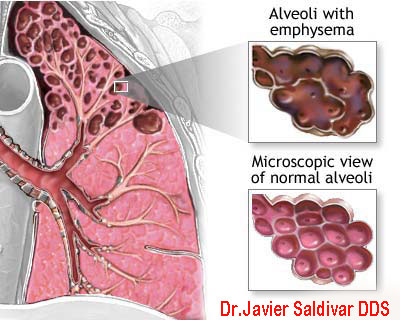
Effect on
Respiratory Disease
Bacteria that
reproduce in the
mouth can also be
carried into the
airways in the
throat and lungs,
increasing the risks
for respiratory
diseases and
worsening chronic
lung conditions,
such as emphysema.
See an
image of
emphysema.
Effect on Pregnancy
Many studies
strongly indicate
that bacterial
infections that
cause moderate-to-severe
periodontal disease
in pregnant women
can increase the
risk for premature
delivery and low
birth weight infants.
The more severe the
infection, the
greater the risk to
the baby. Research
indicates that
bacteria from gum
disease and tooth
decay may trigger
the same factors in
the immune system,
which can then cause
premature dilation
and contractions.
Women should have a
periodontal
examination before
becoming pregnant or
as soon as possible
thereafter. Because
women with diabetes
are at higher risk
for periodontal
disease, it is
especially important
that they see a
dentist early in
pregnancy. Doctors
are still not sure
if treating
periodontal disease
can improve birth
outcomes. In any
case, periodontal
treatment is safe
for pregnant women.
Prevention
Healthy habits and
good oral hygiene
are critical in
preventing gum
disease. Regular and
effective tooth
brushing and mouth
washing, however,
are effective only
above and slightly
below the gum line.
Once periodontal
disease develops,
more intensive
treatments are
needed.
Dietary Changes
It
is important to
reduce both the
quantity and, in
particular, the
frequency of
sugar intake. Avoid
snacks and drinks
with sugar (other
than natural sugars
found in fruits and
vegetables). Eat
sugar-containing
foods with meals,
ideally followed by
brushing. Since
fruit juices can
also cause tooth
erosion in children,
parents should
emphasize milk and
water.
Quitting Smoking
Smoking plays a
significant role in
many cases of
chronic periodontal
disease. For smokers,
quitting is one of
the most important
steps toward
regaining
periodontal health.
Fluoride Treatments
Fluoride treatment
in children has
helped to account
for the decline in
periodontal disease
in adults. Because
fluoride prevents
decay, back molars,
which keep the teeth
in place, are
spared, and are thus
less vulnerable to
bacteria. Even
before teeth first
erupt, babies' gums
should be wiped
clean with a bit of
gauze bearing a dab
of fluoride
toothpaste.
Supplementation with
fluoride tablets or
drops may be
recommended for
children 6 months or
older who drink
unfluoridated water
or who are at risk
for dental problems.
A prescription from
the child's
pediatrician or
dentist is required.
Some dentists
recommend a fluoride
gel for adult
patients who are
still at risk for
tooth decay or
sensitivity, but
extra fluoride is
generally not
necessary for adults
who use fluoride
toothpaste.
Dental Examinations
Periodontitis is a
silent disease.
People with the
disease rarely
experience pain and
may not be aware of
the problem. A
periodontal
examination by a
general dentist once
or twice a year
should reveal any
incipient or
progressive problems.
A full mouth series
of x-rays is advised
every 2 - 3 years.
This will alert the
dentist to early
bone loss and other
disorders of the
oral cavity.
Dentists now often
perform Periodontal
Screening and
Recording (PSR)
using a probe to
measure gum pockets.
Previously performed
only by
periodontists, this
procedure is now
encouraged as part
of a regular dental
examination. The
dentist will
identify any areas
where deep pocketing
has occurred, where
the health of the
gingiva appears
compromised, and
where there is undue
mobility of teeth.
It is the general
dentist's
responsibility to
identify periodontal
disease and inform
the patient. If the
condition is severe,
the dentist may want
to refer the patient
to a periodontist.
Daily
Dental Care
Correct tooth
brushing, mouth
cleansing, and
flossing should be
everyone's defense
against periodontal
disease. (However,
good hygiene is
probably not enough
to prevent
periodontal disease
in many people.
Regular visits to a
dentist are
extremely important,
especially for high-risk
individuals.)
Brushing Guidelines.
The following are
some recommendations
for brushing:
Use a soft-bristled
brush that fits
the size and
shape of your
mouth. Place the
brush where the
gum meets the
tooth, with
bristles resting
along each tooth
at a 45-degree
angle.
Place the brush
where the gum
meets the tooth,
with bristles
resting along
each tooth at a
45-degree angle.
Move the brush
back and forth
gently. Use
short (tooth-wide)
strokes.
Begin by
brushing the
outer tooth
surfaces,
followed by the
inner tooth
surfaces, and
then the chewing
surfaces of the
teeth.
For the inside
surfaces of the
front teeth,
gently use the
tip of the brush
in an up-and-down
stroke.
Brush your
tongue to help
remove
additional
bacteria.
Flossing should
finish the
process. A
mouthwash may
also be used.
If
brushing after each
meal is not
possible, rinsing
the mouth with water
after eating can
reduce bacteria by
30%.
Toothbrushes.
A vast assortment of
brushes of varying
sizes and shapes are
available, and each
manufacturer makes
its claim for the
benefits of a
particular brush.
Look for the
American Dental
Association (ADA)
seal on both
electric and regular
brushes.
In
spite of the wide
variety of
nonelectric
toothbrushes, both
in shape and bristle
design, a study of
eight brands found
no significant
differences in
effectiveness among
them.
Electric
toothbrushes,
particularly those
with a stationary
grip and revolving
tufts of bristles,
can be advantageous
for some people with
physical
disabilities.
Electric
toothbrushes with
heads that move back
and forth up to
thousands of times a
minute remove
significantly more
plaque than ordinary
brushes. Even more
high-tech brushes
are now available
that use sound waves
to remove plaque.
In
general, studies
have reported no
differences between
electric and manual
toothbrushes in
their ability to
remove plaque.
However, if a
regular toothbrush
works, it isn't
necessary to buy an
expensive electric
one.
For individuals with
average dexterity, a
four- or five-rowed,
soft, nylon-bristled
toothbrush is
sufficient. The most
important factor in
buying any
toothbrush, electric
or manual, is to
choose one with a
soft head. Soft
bristles get into
crevices easier and
do not irritate the
gums, thereby
reducing the risk of
exposing teeth below
the gum line
compared to hard
brushes.
Toothbrushes should
be replaced every 1
- 3 months. Not only
do they become
breeding grounds for
bacteria, but the
worn bristles are
less effective at
removing plaque.
Toothpaste.
The objective of a
good toothpaste is
to reduce the
development of
plaque and eliminate
periodontal-causing
microorganisms
without destroying
the organisms that
are important for a
healthy mouth. All
brands should show
ADA approval. Even a
good toothpaste,
however, cannot be
delivered past 3 mm
below the gum line,
where periodontitis
develops.
Toothpastes are a
combination of
abrasives, binders,
colors, detergents,
flavors, fluoride,
humectants,
preservatives, and
artificial
sweeteners. Avoid
highly abrasive
toothpastes,
especially for
individuals whose
gums have receded.
Ingredients
contained in
toothpastes may
include:
Fluoride. Most
commercial
toothpastes
contain fluoride,
which both
strengthens
tooth enamel
against decay
and enhances
remineralization
of the enamel.
Fluoride also
inhibits acid-loving
bacteria,
especially after
eating, when the
mouth is more
acidic. This
antibacterial
activity may
help control
plaque.
Triclosan.
Triclosan is an
anti-bacterial
substance that
may help reduce
mild gingivitis.
Metal salts.
Metal salts,
such as stannous
and zinc, serve
mostly as anti-bacterial
substances in
toothpastes.
Stannous
fluoride gel
toothpastes do
not reduce
plaque, however,
even though they
have some effect
against the
bacteria that
cause it, but
slightly reduce
gingivitis.
Peroxide and
baking soda.
Toothpastes with
these
ingredients
claim to have a
whitening action,
but while they
may help remove
stains there is
little evidence
they whiten the
actual color of
the teeth. In
addition, these
substances
appear to offer
no benefits
against gum
disease.
Antibacterial
sugar
substitutes (xylitol),
and detergents (delmopinol)
Mouthwashes.
The American Dental
Association
recommends (in
addition to daily
brushing and
flossing)
antimicrobial
mouthwash to help
prevent and reduce
plaque and
gingivitis, and
fluoride
mouthwashes to help
provide additional
protection against
tooth decay.
Chlorhexidine (Peridex
or PerioGard) is
an antimicrobial
mouthwash
available by
prescription
only. It reduces
plaque by 55%
and gingivitis
by 30 - 45%.
Patients should
rinse for 1
minute twice
daily. They
should wait at
least 30 minutes
(and preferably
2 hours) between
brushing and
rinsing since
chlorhexidine
can be
inactivated by
certain
compounds in
toothpastes. It
has a bitter
taste. It also
binds to tannins,
which are in
tea, coffee, and
red wine, so it
has tendency to
stain teeth in
people who drink
these beverages.
Studies are
mixed as to its
effectiveness
for preventing
or reducing
periodontal
disease.
Listerine is
another
antimicrobial
mouthwash. It is
composed of
essential oils
and is available
over the counter.
It reduces
plaque and
gingivitis, when
used for 30
seconds twice a
day. It leaves a
burning
sensation in the
mouth that most
people better
tolerate after a
few days of use.
The usual
regimen is to
rinse twice a
day. (Listerine
PocketPaks,
which are strips
that dissolve on
the tongue, have
no proven
effects on
plague and
gingivitis.)
Mouthwashes
containing
cetylpyridinium
(Scope, Cepacol)
have moderate
antimicrobial
effect on
plaque, but only
if they are used
an hour after
brushing. None
are as effective
as Listerine or
chlorhexidine,
but they may
still have some
value for people
who cannot
tolerate the
other
mouthwashes.
Mouthwashes
containing
stannous
fluoride and
amine fluoride (Meridol)
are moderately
effective, but
are also not as
effective as
effective as
Listerine or
chlorhexidine.
Fluoride
mouthwashes
(Act) are
helpful in
preventing
cavities.
Mouthwashes that
contain alcohol
are dangerous
for children and
should be kept
away from them.
Flossing.
The use of dental
floss, either waxed
or unwaxed, is
critical in cleaning
between the teeth
where the toothbrush
bristles cannot
reach. In spite of
this, nearly
two-thirds of people
do not floss.
To
floss correctly, the
following steps may
be helpful:
Break off about
18 inches of
floss and wind
most of it
around the
middle finger of
one hand and the
rest around the
other middle
finger.
Hold the floss
between the
thumbs and
forefingers and
gently guide and
rub it back and
forth between
the teeth.
When it reaches
the gum line,
the floss should
be curved around
each tooth and
slid gently back
and forth
against the gum.
Finally, rub
gently up and
down against the
tooth. Repeat
with each tooth,
including the
outside of the
back teeth.
If, on repeated
flossing
attempts, the
floss becomes
shredded or
cannot be
removed easily
from between the
teeth, a rough
crown or
overhanging
filling may be
the cause. In
such cases, the
restoration
should be redone.
Such areas
create spaces
for the
collection of
food debris,
plaque, and
calculus.
Here are some tips
in choosing the
right floss or
flossing device:
Use a floss that
does not shred
or break.
Avoid a very
thin floss,
which can cut
the gum if
brought down
with too much
force or not
guided along the
side of the
tooth.
A
floss threader
is an invaluable
aid for the
person who has
bridgework. Made
of plastic, it
looks like a
needle with a
huge eye, or
loop. A piece of
floss is
threaded into
the loop, which
can then be
inserted between
the bridge and
the gum. The
floss that is
carried through
with it can then
be used to clean
underneath the
false tooth or
teeth and along
the sides of the
abutting teeth.
Another handy
device for
cleaning under
bridges is a
Proxabrush,
which is an
interdental
cleaner. This is
a tiny narrow
brush that can
be worked in
between the
natural teeth
and around the
attached false
tooth or teeth.
Special
toothpicks such
as Stim-U-Dent
may be effective
for wide spaces
between teeth
but should never
replace
flossing.
Standard
toothpicks
should never be
used for regular
hygiene.
Electronic
products, such
as water piks,
are also
helpful. These
devices are
expensive but
may improve
flossing
compliance.
Producing Saliva and
Drinking Water.
Saliva is important
for diluting the
toxins created by
plaque. Drinking at
least 7 glasses of
water a day helps
reduce inflammation
in the mouth by
producing more
saliva. Increasing
water intake is
particularly
important as one
ages, when less
saliva is produced.
Diagnosis
The dental
practitioner
typically performs a
number of procedures
to determine a
diagnosis of
periodontal disease.
Medical History
The dentist will
first take a medical
history to reveal
any past or present
periodontal problems,
any underlying
diseases that might
be contributing to
the problem, and any
medications the
patient is taking.
After noting the
general state of
oral hygiene, the
dentist may ask
about the quality of
home dental care.
Physical Examination
Inspection of the
Gum Area.
The dentist inspects
the color and shape
of gingival tissue
on the cheek (buccal)
side and the tongue
(lingual) side of
every tooth and
compares these
qualities to the
healthy ideal.
Redness, puffiness,
and bleeding upon
probing indicate
inflammation. If the
gum formation
between teeth is
blunt and not
pointed, acute
necrotizing
periodontal disease
may be indicated.
Periodontal
Screening and
Recording (PSR).
PSR is a painless
procedure used to
measure and
determine the
severity of
periodontal disease:
The dentist uses
a mirror and a
periodontal
probe, a fine
instrument
calibrated in
millimeters (mm),
which is used to
measure pocket
depth.
The probe is
held along the
length of the
tooth with the
tip placed in
the pocket. The
tip of the probe
will then touch
the point where
the connective
tissue attaches
to the tooth.
The dentist will
"walk" the probe
to six specified
points on each
tooth, three on
the buccal
(cheek) and
three on the
lingual (tongue)
sides. The
dentist measures
the depth of the
probe at each
point.
Pocket depths
greater than 3
mm indicate
disease.
These measurements
help determine the
condition of the
connective tissue
and amount of
gingival overgrowth
or recession.
Testing Tooth
Movement.
Tooth mobility is
determined by
pushing each tooth
between two
instrument handles
and observing any
movement. Mobility
is a strong
indicator of bone
support loss.
X-rays.
X-rays are taken to
show any loss of
bone structure
supporting the
teeth. Eighteen
x-rays make up the
full mouth series
necessary for
diagnosis.
Treatment
Studies support the
effectiveness of
active treatment
combined with a
strict maintenance
program for patients
with periodontal
disease. In one
study, for example,
people with
periodontal disease
who were
inconsistent in
caring for their
gums after treatment
had nearly six times
the risk for tooth
loss as those who
were very vigilant.
Some dentists have
reported a success
rate of 85% when
professional
treatment and good
home maintenance are
combined. Treatment
helps nonsmokers
more than smokers,
particularly when
pockets are deep and
persistent. Some
studies suggest that
periodontal
treatment in people
with type 2 diabetes
helps improve blood
sugar levels.
Whether treatment
will help reduce
other health risks,
including heart
attack and stroke,
is unknown.
Treatment Goals.
Once periodontal
disease has been
identified, the
goals of treatment
are:
To arrest and
control the
progress of the
disease
To leave the
periodontal
tissues in an
easily
maintainable
state
If possible, to
restore the
supporting
structures,
which include
bone, gum
tissue, and
ligaments
Treatment Phases.
To achieve these
goals, there are
various approaches:
Initial
cleaning,
scaling, and
curettage
Surgery -- if
needed for
reducing deep
pockets that
remain
underneath the
gum after
extensive
cleaning
sessions
Low-dose oral or
topical
antibiotics
Maintenance
After the active
treatment is
completed and the
mouth is in a
relative state of
health, the patient
should have regular
cleanings lasting 45
minutes to 1 hour,
about every 3 months.
These may be done by
the dental hygienist,
the periodontist, or
the general dentist.
The patient may
alternate between
them. Home care, of
course, must be
continued.
Antibiotics Before
Treatment.
In cases where the
individual has a
mitral valve
prolapse or history
of rheumatic heart
disease,
pretreatment with an
appropriate
antibiotic is
required before any
dental work,
including cleaning.
This is necessary to
prevent the
possibility of
bacterial
endocarditis, which
can be life
threatening.
Deep
Cleaning: Scaling
and Root Planing
Scaling, polishing,
and sometimes
curettage are used
to manage
periodontal disease.
They are usually
accomplished in a
series of three to
four visits spaced
about a week apart.
(Patients might ask
their dentist about
the gas nitrous
oxide, which is
helpful for many
patients and may
reduce the visits to
a single one.) The
dental hygienist or
practitioner
generally uses both
ultrasonic and
manual instruments
to remove calculus.
Calculus above
the gum is
easily seen. The
dental
professional
usually detects
calculus below
the gum by
careful probing
with an
instrument.
The hygienist or
dentist may use
an ultrasonic
instrument for
removal of the
more accessible
calculus. This
probe-like
device vibrates
at a frequency
range higher
than is audible
to the human ear.
Some people with
low tolerance
for the
ultrasonic probe
may wish to
request nitrous
oxide.
A
spray of water
is used with
ultrasound to
prevent
overheating and
to flush out the
debris that is
dislodged.
The dental
professional
will scrape the
plaque from
above and below
the gum line (called
scaling). When
the probe
contacts the
rock-like
calculus,
deposits
fracture off the
tooth fairly
efficiently.
The hygienist or
dentist will
then smooth the
rough spots on
the tooth.
Smoothing the
surface helps
remove bacteria
that collect
there (root
planing) and
also helps the
gums reattach.
Polishing is the
finishing
procedure. It
uses a rubber
cup with an
abrasive paste
to remove plaque
and stains on
the crown
portion of the
tooth. It
produces a
smooth surface,
making it
temporarily
harder for
plaque to adhere.
After the cleaning
procedure, the
dentist will check
the pocket depths
around the teeth
after the cleaning
process has been
completed. Further
treatment needs are
determined by the
results of these
initial sessions:
If the cleaning
processes have
reduced
inflammation,
observation only
is needed.
If an abscess is
present, surgery
may be required.
Finally, the dental
hygienist or
practitioner should
offer thorough
instructions on home
care to insure the
removal of bacteria
on a daily basis.
This includes proper
use of the
toothbrush, paste,
mouth rinses, floss,
floss threaders, and
proxabrushes. Home
care can effectively
eliminate the plaque
above the gums and
down to 2 mm below
the gums.
Gingival Curettage
Gingival curettage
removes the soft
tissue lining of the
periodontal pockets
in order to
completely eliminate
bacteria and
diseased tissue. It
may be used along
with scaling and
root planing, but
achieves a deeper
and more complete
cleaning. Evidence
indicates, however,
that it does not
contribute any
additional benefits
beyond simple
scaling and planing.
Surgery (Open Flap
Curettage)
Surgery allows
access for deep
cleaning of the root
surface, removal of
diseased tissue, and
repositioning and
shaping of the bones,
gum, and tissues
supporting the teeth.
Surgical procedures
vary depending on
the individual
diagnosis and needs
of the patient. The
basic procedure is
known as open flap
curettage. It
involves:
The periodontal
surgeon lifts,
or flaps, the
gums away from
the tooth and
surrounding bone.
The diseased
root surfaces
are cleaned and
curetted
(scraped) to
remove deposits.
Gum tissue is
replaced into
positions to
minimize pocket
depth.
The periodontist
may also contour
the remaining
bone and attempt
to regenerate
lost bone and
gingival
attachment
through bone
grafts and
guided tissue
regeneration or
the use of
enamel matrix
protein
derivatives.
There is some debate
about whether this
procedure is any
more effective in
preventing disease
progression than
non-surgical
therapies, such as
low-dose
doxycycline,
short-term
antibiotics, or
antibiotic gels.
Some studies have
reported that
although surgical
treatment reduced
pocket depth more
than non-surgical
therapies for at
least a year after
the procedure,
benefits from
surgery do not
persist beyond 5
years, except in
very deep pockets.
Postsurgery Pain and
Discomfort.
Post-surgery
discomfort is
usually managed
easily with
over-the-counter
medications such as
ibuprofen. If
discomfort is
severe, stronger
analgesics may be
prescribed. Some
patients experience
sensitivity to hot
or cold temperatures
from exposed roots.
These problems can
be managed with
topical fluoride
treatments or, in
severe cases, with
dental restoration.
Techniques and
Materials for
Restoring Gum Tissue
and Bone
Guided Tissue
Regeneration.
A more advanced
technique, called
guided tissue
regeneration, is
used to stimulate
bone and gum tissue
growth:
First, the root
surfaces and
diseased bone
are meticulously
cleaned out.
Preventing
bacterial
contamination is
very important.
The more
residual
bacteria, the
greater the
chance that the
treatment will
fail.
A
specialized
piece of fabric
is sewn around
the tooth to
cover the crater
in the bone left
after the
cleaning. It is
either
absorbable or
nonabsorbable.
The gum is then
sewn over the
fabric. The
fabric prevents
the gum tissue
from growing
down into the
bone defect and
allows the bone
and the
attachment to
the root to
regenerate.
After 4 - 6
weeks, the
nonabsorbable
fabric must be
removed using a
minor surgical
procedure. The
absorbable
membrane may be
left in. In
general, there
is little
difference in
outcome between
absorbable and
nonabsorbable
procedures. The
absorbable
fabric may not
be as effective
as standard
grafts if gum
tissue is thin,
although newer
materials may
prove to produce
better results.
Bone
Grafting.
In some cases of
severe bone loss,
the surgeon may
attempt to encourage
regrowth and
restoration of bone
tissue that has been
lost through the
disease process.
This involves bone
grafting:
The surgeon
places bone
graft material
into the defect.
The material may
be either bone
from the same
patient or a
substance called
decalcified
freeze-dried
bone allografts
(DFDBA) which is
obtained from a
donor.
This material
then stimulates
new bone growth
in the area.
Enamel Matrix
Protein Derivative.
Amelogenin is a
derivative of a
major protein in the
structure (the
matrix) of enamel
that helps stimulate
gum tissue growth. A
gel containing
amelogenin
(Emdogain) is
applied during
surgery and forms a
coat over the roots
of the teeth. The
gel itself dissolves
after 2 days,
leaving the active
substance behind.
Studies report that
it is safe and may
significantly reduce
the effects of
periodontal disease.
Cosmetic and Gum
Grafting Treatments
Gum grafting
techniques can also
be very useful for
improving the looks
of the gum as well
as adding support to
the teeth. During
this procedure, the
periodontist takes
gum tissue from the
palate or another
donor source to
cover the exposed
root in order to
even the gum line
and reduce
sensitivity. Other
procedures are
available to improve
the look of the gums
and teeth. The gum
line can be sculpted
to improve uneven or
excess gums and to
cover exposed roots
as gums recede.
Implants
Periodontists report
that they are
achieving great
success with tooth
implants in patients
who have lost teeth
due to periodontal
disease. The average
cost for a single
implant is high,
however, and one
implant requires 5 -
7 months for
completion.
Medications
Antibiotics are
often used in
combination with
surgery, curettage,
or alone to
eliminate or prevent
disease-causing
bacteria after
periodontal
procedures. They are
being investigated
in oral forms as
well as in topical
forms that are
applied directly to
the gum.
Increasingly, dental
professionals are
finding that local
application of
antibiotics is more
effective than
periodontal surgery
alone. They may even
prove to be an
alternative to
surgery.
Oral
Antibiotics at
Standard Doses
Antibiotics given
orally and at
standard doses have
some limited
applications for
periodontal disease.
They are typically
given for an acute
infection. Long-term
use of antibiotics
is advised for the
control of juvenile
periodontitis,
refractory
periodontitis,
rapidly progressing
periodontitis, and
prepubertal
periodontitis.
(Long-term use of
oral antibiotics is
generally not
advised due to the
risks of bacterial
resistance.)
Specific antibiotics
used in periodontal
disease include:
Tetracycline
antibiotics --
which include
tetracycline
hydrochloride,
doxycycline, and
minocycline --
are the primary
drugs used. They
not only have
anti-bacterial
actions but also
reduce
inflammation and
help block
collagenase, the
protein that
destroys
connective
tissue and bone,
even in low
doses. In fact,
these two
actions seem to
contribute most
to periodontal
protection,
rather than
their
antibacterial
properties.
Short-term use
of standard-dose
doxycycline (a
10-day
treatment) is
used for
treating acute
periodontal
infections and
for eliminating
inflammation.
Topical
application and
long-term use of
these
antibiotics are
showing
particular
promise.
Some macrolide
antibiotics
(roxithromycin)
may have actions
against
inflammation and
growth involved
in periodontal
disease.
Some quinolone
antibiotics
(moxifloxacin,
ciprofloxacin)
may specifically
target A.
actinomycetemcomitans,
an important
bacteria in
periodontal
disease.
Metronidazole
(Flagyl) in
combination with
tetracycline or
amoxicillin (a
penicillin) may
be used for
severe and
chronic
periodontal
disease.
Direct Delivery of
Antibiotics to the
Gums
Topical application
of antibiotics to
the gum surface does
not affect the
entire body like
oral antibiotics do,
and they are
preferred whenever
possible. Studies
suggest that, in
combination with
scaling and planing,
any of these
approaches are very
effective for
periodontal health.
Low-Dose and
Chemically Modified
Tetracyclines
Subantimicrobial
Dose Doxycycline
(Periostat).
Subantimicrobial
dose doxycycline
(SDD) is a term used
for a treatment that
uses very low doses
(20 mg) of
doxycycline
(Periostat).
Although doxycycline
is a tetracycline
antibiotic, the
doses used are too
low to affect
bacteria. However,
at these dose
levels, the drug
blocks matrix
metalloproteinases
(MMPs) -- enzymes
that destroy the
connective tissues
holding the teeth.
Periostat is taken
twice a day for
months.
There is some
concern that such
long-term use may
pose a risk for the
development of
antibiotic-resistant
bacteria or other,
still unknown,
adverse effects. The
doses used in this
treatment, however,
are too low to have
any effect on
bacteria, so this
risk may be very
low. In fact,
several 12-month
studies report
significant
improvements in
tooth attachment and
pocket depth with no
increased incidence
of side effects.
[Taking a common
nonsteroidal
anti-inflammatory
drug, such as
aspirin or ibuprofen
(Advil) along with
doxycycline, may
enhance the
effectiveness of
this treatment.]
Chemically Modified
Tetracyclines.
Other tetracyclines
are being developed
that inhibit MMPs
but have no
antibiotic
properties, which
would, theoretically,
avoid possible long-term
problems with
antibiotic
resistance.
Nonsteroidal Anti-Inflammatory
Drugs (NSAIDs)
NSAIDs are drugs
that block factors
that cause
inflammation and
pain.
These drugs are used
not only for
relieving pain in
periodontal disease
but also for slowing
the disease process.
NSAIDs block
inflammatory enzymes
triggered by
cytokines, which are
important immune
factors in
periodontal disease.
A number of NSAIDs
are being
investigated for
their benefits in
reducing gingivitis
and slowing
progression of
periodontal disease.
Investigators are
also studying rinses,
creams, and other
topical forms of
NSAIDs. Long-term
use of NSAIDs can
cause stomach
problems, such as
ulcers and bleeding,
and possible heart
problems.



 La
Periodoncia es una rama de la Odontología que se encarga del estudio
y tratamiento de los tejidos que rodean y dan soporte a los dientes;
Existen múltiples alteraciones que pueden afectar a estos tejidos,
entre los más comunes está la gingivitis (inflamación crónica de las
encías), y la periodontitis (pérdida parcial o total del hueso
soporte). Los tratamientos periodontales actuales utilizan un sin
número de nuevas técnicas y materiales que permiten conservar los
dientes por más tiempo y en mejores condiciones.
La
Periodoncia es una rama de la Odontología que se encarga del estudio
y tratamiento de los tejidos que rodean y dan soporte a los dientes;
Existen múltiples alteraciones que pueden afectar a estos tejidos,
entre los más comunes está la gingivitis (inflamación crónica de las
encías), y la periodontitis (pérdida parcial o total del hueso
soporte). Los tratamientos periodontales actuales utilizan un sin
número de nuevas técnicas y materiales que permiten conservar los
dientes por más tiempo y en mejores condiciones.




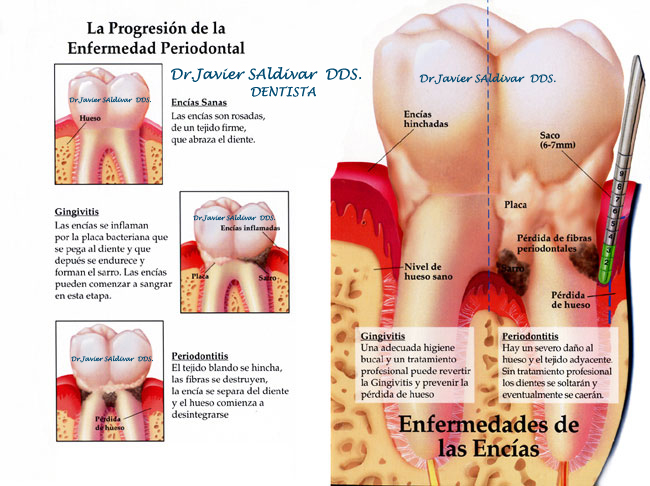
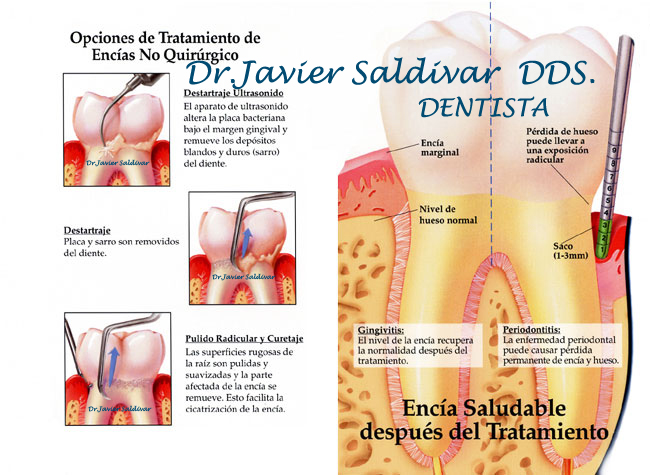
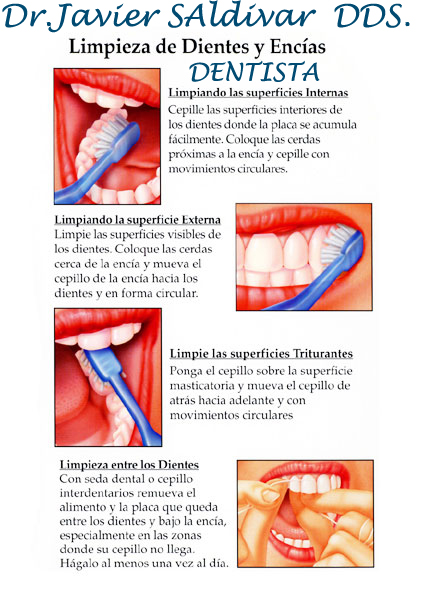
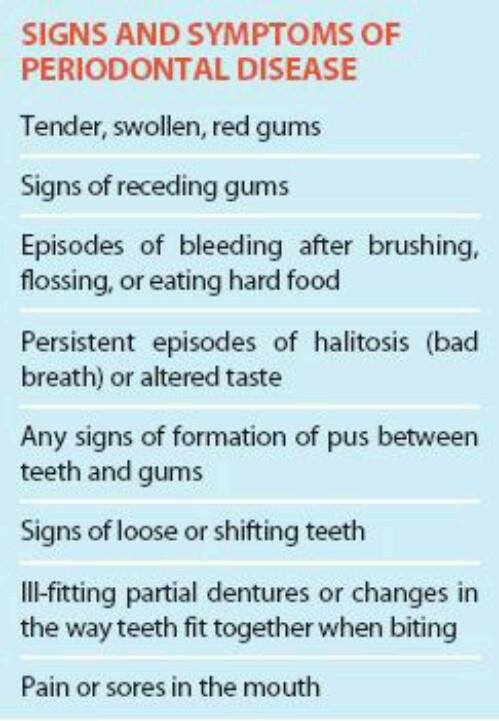

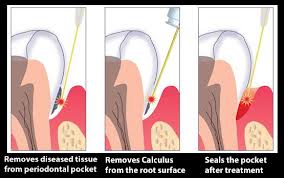
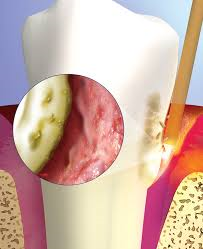

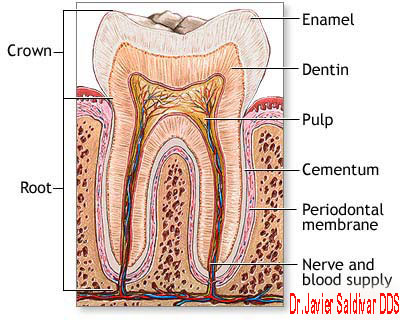
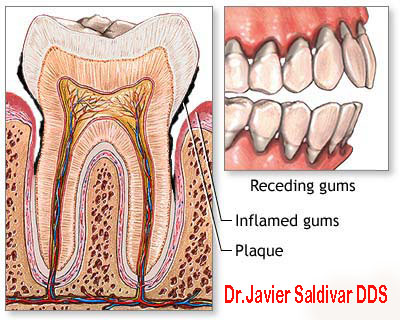
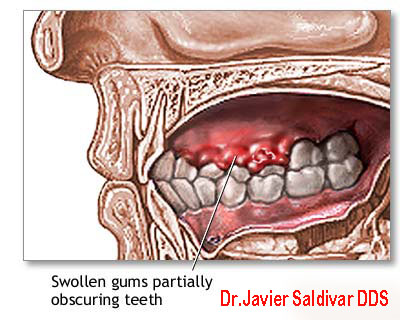
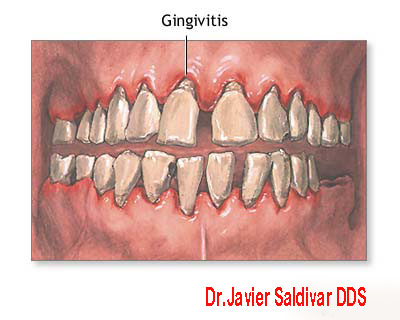
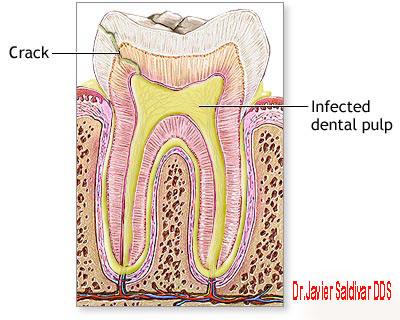 Pain is usually not
a symptom, which
partly explains why
the disease may
become advanced
before treatment is
sought and why some
patients avoid
treatment even after
periodontitis is
diagnosed.
Pain is usually not
a symptom, which
partly explains why
the disease may
become advanced
before treatment is
sought and why some
patients avoid
treatment even after
periodontitis is
diagnosed.