|
|



Copyright © 2018 Dr.Javier Saldivar V. All Rights Reserved.
|
The average adult has thirty-two teeth by age eighteen: Wisdom Teeth Wisdom teeth are actually the 3rd molars. They develop inside the bone (as all other teeth do) beginning at age 9. These teeth are the last to form and the farthest back.
For these reasons, most often, I advise patients to have their wisdom teeth removed. Teeth all form the crown first and then the roots form and grow to length. For this reason I recommend that the wisdom teeth be removed sooner rather than later (before the roots fully form). Most people believe that the wisdom teeth will push the other teeth forward (especially on the lower) and cause crowding to occur in the front teeth. I do not believe this is the case, rather, I believe that the crowding that occurs is due to other factors. About wisdom teeth removalWisdom teeth usually emerge from the gum between the ages of 17 and 24. They are the last of the large grinding teeth at the back of the mouth (molars). Some people never develop wisdom teeth but you could have up to four - one in each corner of your mouth.
Wisdom teeth are easier to remove when the patient is younger, since their roots are not completely formed, the surrounding bone is softer, and there is less chance of damaging nearby nerves or other structures. Removal of wisdom teeth at a later age becomes more complicated as the roots have fully developed (may involve the nerve), and the jawbone is denser.
Wisdom teeth don't usually cause any problems and so don't need to be removed. However, if there isn't enough space for them to grow at the back of your mouth (impacted wisdom teeth), they can cause pain, swelling or infection.
Having your impacted wisdom teeth surgically removed (extracted) can help relieve your symptoms. It may be possible for your dentist to remove your wisdom teeth or he or she may refer you to a dental surgeon.
What are the alternatives?Antibiotics can help treat an infection, but symptoms tend to flare up again. Having wisdom teeth removed is often the only way to permanently relieve your symptoms. Preparing for your operationYour surgeon or dentist will explain how to prepare for your operation. For example, if you smoke you will be asked to stop, as smoking increases your risk of getting a wound infection and slows your recovery. The operation is usually done as a day case under local anaesthesia. This completely blocks feeling in the gum and you will stay awake during the operation. Your surgeon or dentist will advise which type of anaesthesia is most suitable for you. About the operationOnce the anaesthetic has taken effect, your dentist or surgeon will cut through your gum and may remove some of your jawbone to reach the tooth. The tooth is removed and the wound is closed with stitches. Most wisdom teeth only take a few minutes to remove but more difficult wisdom teeth can take up to 60 minutes. What to expect afterwardsAfter a local anaesthetic it may take several hours before the feeling comes back into your jaw. Take special care not to bump or knock the area. You will be able to go home when you feel ready. You may be given painkillers, antibiotics and mouthwash solutions to take home. You may also be given a date for a follow-up appointment. Dissolvable stitches will disappear on their own in seven to 10 days. Non-dissolvable stitches are removed a week after surgery. Recovering from wisdom teeth removalIf you need them, you can take over-the-counter painkillers such as paracetamol or ibuprofen. Follow the instructions in the patient information leaflet that comes with your medicine. Don't vigorously rinse out your mouth during the first 24 hours after having a wisdom tooth removed because this can disturb blood clots that help the healing process. After meals you can rinse gently with warm salt water (half a teaspoon of table salt dissolved in a glass of water). You should brush your teeth as usual, but keep your toothbrush away from the healing wound for the first couple of days. At first, you may feel small fragments of bone with your tongue. These are the edges of the tooth socket and will soon disappear as the gum heals. Eating and drinkingTo begin with, you should eat soft foods, gradually returning to a normal diet once your jaw feels less stiff. BleedingIf your gum bleeds, fold a clean handkerchief or piece of gauze, place it on the bleeding gum and bite on it for at least 20 minutes. Don't rinse your mouth out or lie down until the bleeding has stopped. Most people don't experience any problems after having their wisdom teeth removed. However, contact your dentist or your GP immediately if you develop any of the following symptoms:
What are the risks?Wisdom teeth removal is commonly performed and generally safe. However, in order to make an informed decision and give your consent, you need to be aware of the possible side-effects and the risk of complications of this procedure. Side-effectsYou may have some facial swelling, pain, jaw stiffness and some bleeding for up to two weeks. These symptoms are usually at their worst for the first two or three days and then gradually improve. ComplicationsThis is when problems occur during or after the operation. Most people are not affected. The possible complications of any operation include an unexpected reaction to the anaesthetic or excessive bleeding. Specific complications of having wisdom teeth extracted are uncommon but may include:
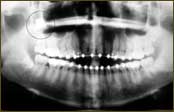
The exact risks are specific to you and will differ for every person, so we have not included statistics here. Ask your surgeon or dentist to explain how these risks apply to you. Wisdom Teeth Extractions. Third molars, commonly referred to as wisdom teeth, are usually the last four of 32 teeth to erupt (surface) in the mouth, generally making their appearance between the ages of 17 to 25. They are located at the back of the mouth (top and bottom), near the entrance to the throat. The term “wisdom” stems from the idea that the molars surface at a time typically associated with increased maturity or “wisdom”. In most cases, inadequate space in the mouth does not allow the wisdom teeth to erupt properly and become fully functional. When this happens, the tooth can become impacted (stuck) in an undesirable or potentially harmful position. If left untreated, impacted wisdom teeth can contribute to infection, damage to other teeth, and possibly cysts or tumors. There are several types, or degrees, of impaction based on the actual depth of the teeth within the jaw: Tissue Impaction:ace"> The upper portion of the tooth (the crown) has penetrated through the bone, but the gingiva (gum) is covering part or all of the tooth’s crown and has not positioned properly around the tooth. Because it is difficult to keep the area clean, food can become trapped below the gum and cause an infection and/or tooth decay, resulting in pain and swelling. Partial Bony Impaction:The tooth has partially erupted, but a portion of the crown remains submerged below the gum and surrounding jawbone. Again, because it is difficult to keep the area clean, infection will commonly occur. Complete Bony Impaction:The tooth is completely encased by jawbone. This will require more complex removal techniques. Reasons to remove wisdom teeth While not all wisdom teeth require removal, wisdom teeth extractions are most often performed because of an active problem such as pain, swelling, decay or infection, or as a preventative measure to avoid serious problems in the future. If impaction of one or more wisdom teeth is present, and left untreated, a number of potentially harmful outcomes can occur, including: Damage to nearby teeth: Second molars (the teeth directly in front of the wisdom teeth) can be adversely affected by impacted wisdom teeth, resulting in tooth decay (cavities), periodontal disease (gum disease) and possible bone loss. Disease: Although uncommon, cysts and tumors can occur in the areas surrounding impacted wisdom teeth. Infection: Bacteria and food can become trapped under the gum tissue, resulting in an infection. The infection can cause considerable pain and danger. Tooth Crowding: It has been theorized that impacted wisdom teeth can put pressure on other teeth and cause them to become misaligned (crowded or twisted). This theory isn’t universally accepted by all dental professionals, and it has never been validated by any scientific studies. Wisdom teeth examination As with any dental procedure, your dentist will want to initially conduct a thorough examination of the wisdom and surrounding teeth. Panoramic or digital x-rays will be taken in order for your dentist to evaluate the position of the wisdom teeth and determine if a current problem exists, or the likelihood of any potential future problems. The x-rays can also expose additional risk factors, such as deterioration or decay of nearby teeth. Early evaluation and treatment (typically in the mid-teen years) is recommended in order to identify potential problems and to improve the results for patients requiring wisdom teeth extractions. Only after a thorough examination can your dentist provide you with the best options for your particular case.
Copyright © 2018 Dr.Javier Saldivar V. All Rights Reserved. |
 12 years
12 years 14
years
14
years 17
years
17
years 24
years
24
years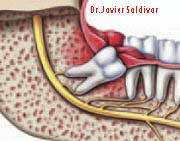 Infection
Infection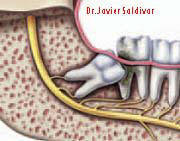 Crowding,
damage
Crowding,
damage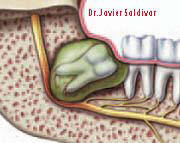 Cyst
Cyst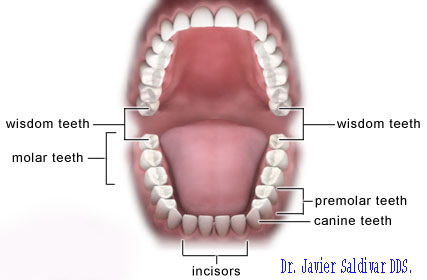

| ¿Por qué se deben extraer los 3eros molares? |
|
Cuando no existe ninguna posibilidad de tratamiento conservador de un diente, es necesario recurrir a su extracción. Con frecuencia las extracciones son temidas por el paciente incluso más que otras intervenciones quirúrgicas no relacionadas con la boca. El avance de las modernas técnicas de anestesia local hace que en la actualidad las extracciones puedan ser realizadas sin ningún tipo de dolor y con el menor grado de molestia para el paciente. Por otro lado, si hay cierto grado de miedo a la intervención existen una gran variedad de fármacos que permiten que el paciente esté relajado durante el acto operatorio y no esté en tensión o con nerviosismo. La causa más frecuente por la que debe ser extraído un diente es la destrucción por caries, y es un segundo lugar la causante es la enfermedad periodontal (la piorrea). Sin embargo, existen otras situaciones en las que es precisa la extracción de un diente, aunque son menos frecuentes que las dos anteriores: · Dientes fracturados: Cuando se produce un traumatismo en la cara puede ocurrir que alguno de nuestros dientes sean afectados. Si esta fractura o rotura se produce en la raíz, por debajo de la encía, no es posible restaurar el diente o muela, por lo que hay que extraerla. · Extracción de dientes sanos para realizar tratamientos de ortodoncia. Ante una mal posición de los dientes que necesiten ser alineados mediante un tratamiento ortodóncico, puede ocurrir que haya una importante falta de espacio. En estos casos la única manera de conseguir espacio suficiente para la correcta colocación de nuestros dientes es la extracción de alguna pieza dental, generalmente los primeros premolares. · Extracción de dientes para facilitar la construcción de una prótesis. Un diente o muela en una mala posición puede dificultar la colocación de una prótesis para poder rehabilitar los maxilares. · Dientes temporales retenidos. Si los dientes deciduos o "de leche" no se recambian a su debido tiempo, pueden provocar una alteración en la posición o erupción de los dientes definitivos, por lo que deben ser extraídos. · Dientes incluidos (no erupcionados). Los dientes incluidos son dientes que no han erupcionados durante su período normal de erupción. En estos casos debemos descartar cualquier tipo de patología y realizar una radiografía panorámica para poder determinar la causa en este retraso de la erupción. Las inclusiones más frecuentes son las 3eras molares (muelas del juicio) superiores o inferiores y la de los caninos (colmillos), sobre todo en el maxilar superior. Los problemas en la erupción de los 3eros molares es muy frecuente, y esto es debido a que en la evolución del hombre, el tamaño del maxilar superior y de la mandíbula ha ido disminuyendo más rápidamente que le número de dientes. Esto produce una falta de espacio que impide la normal erupción de éstos. En su intento por salir, los cordales, empujan al resto de dientes que ya están colocados en la arcada, pudiendo provocar apiñamiento y mal posición de los mismos. De igual manera, los intentos de erupción de estas muelas provocan episodios de dolor, inflamación y supuración. Los caninos incluidos generalmente presentan una falta de espacio en la arcada o bien su posición dentro del hueso es incorrecta. En la mayoría de casos el diente "de leche" permanece incluso hasta edad adulta, ya que no es empujado por el definitivo. Por otra parte, el canino incluido puede lesionar las raíces de los dientes cercanos a él e incluso provocar su caída. La importancia de extraer los dientes o muelas incluidas radica en que estos dientes son una bomba de tiempo, que pueden empezar a dar problemas en cualquier momento. Y siempre es mejor realizar la extracción o cirugía, cuando no existe sintomatología ni molestias, ya que el postoperatorio es mejor.
Copyright © 2018 Dr.Javier Saldivar V. All Rights Reserved. |

|
 TERCEROS MOLARES Y DIENTES RETENIDOS Los dientes retenidos son aquellos que por diferentes razones no erupcionaron o no encontraron suficiente espacio en los maxilares. De todos los que más comúnmente requieren su extracción quirúrgica son los terceros molares. También llamadas muelas del juicio, estas son los últimos dientes en
erupcionar en la boca. Estas cuatro muelas no siempre tienen espacio, pues
en ocasiones son muy grandes para un lugar reducido o están orientadas en
mala dirección, por lo que al intentar erupcionar pueden mover otros
dientes. Por ser las más posteriores en la cavidad bucal, su limpieza se
dificulta y es muy común que provoquen infecciones. |
||
 |
 |
||
¿CUANDO DEBEN EXTRAERSE? El periodo de erupción normal es entre los 14 y los 24 años, por lo que por medio de radiografías se puede saber su posición, y así realizarse el tratamiento antes de que causen problemas. Es recomendable que las extracciones se hagan entre esas edades o inclusive antes. Para su extracción en ocasiones se realiza una pequeña cirugía donde se corta encía, hueso y a veces se divide la muela, para poderla extraer. El Cirujano Dentista debe tener los conocimientos y la experiencia
para realizar la cirugía y extracción de dientes retenidos, reduciendo así
el tiempo quirúrgico, disminuyendo el trauma y con esto la recuperación es
mejor. |
|||

|
 |
||


|
Muelas del Juicio o Cordales Las muelas del juicio son las 3eras molares y son cuatro. Se forman adentro de la mandíbula o maxilar (como las otras piezas dentales) Se principian a formar a los 9 años. Estas muelas son las ultimas en formarse y en salir y se encuentran al final.
|
|
Usted es genéticamente afortunado, Si su mandíbula es lo suficientemente larga para acomodar las 3eras molares en una posición correcta para su erupción, su limpieza y su uso en la masticación. |
 |
|
Por lo regular, las mandíbulas no son lo suficientemente largas para poder alojar a las muelas del juicio.A esto se le llama muelas impactadas (atrapadas) en la mandibula. |
 |
|
Si la muela del juicio erupciona parcialmente por la encía, las bacterias se alojaran debajo de la encía alrededor de la corona. Y como esa es una área casi imposible de poder limpiar se comenzara a formarse una infección. |
 |
|
Algunas veces la infección es tan intensa que se puede infectar el hueso. |
 |
|
Es posible que la muela del juicio cause destrucción de la muela vecina (2do molar). |
 |
|
Por esas razones recomendamos a nuestros pacientes la cirugía de sus muelas el juicio .Entre mas pronto mejor.(Se recomienda extraerlas antes de la formación total de las raíces)
|
 Debido
a procesos evolutivos del ser humano o a diferencias de tamaño entre los huesos
maxilares y el tamaño de las piezas dentarias, los terceros molares no siempre
logran erupcionar completamente (emerger en la boca), lo que genera un espacio
de difícil acceso en la zona posterior de la cavidad bucal, el cual acumula
restos de alimentos y placa bacteriana difícil de asear. Al inflamarse la zona
se produce un cuadro infeccioso llamado pericoronarítis, la cual, puede ser
aguda o crónica y conducir a infecciones graves incluso que pueden comprometer
la vida del paciente.
Debido
a procesos evolutivos del ser humano o a diferencias de tamaño entre los huesos
maxilares y el tamaño de las piezas dentarias, los terceros molares no siempre
logran erupcionar completamente (emerger en la boca), lo que genera un espacio
de difícil acceso en la zona posterior de la cavidad bucal, el cual acumula
restos de alimentos y placa bacteriana difícil de asear. Al inflamarse la zona
se produce un cuadro infeccioso llamado pericoronarítis, la cual, puede ser
aguda o crónica y conducir a infecciones graves incluso que pueden comprometer
la vida del paciente.  porcentaje
de dientes retenidos que la raza negra, ya que en esta última, el desarrollo y
dimensiones de los maxilares son mayores. Se plantea un hecho establecido en
genética que en realidad se hace ley. Un individuo puede heredar los maxilares
pequeños de un progenitor y los dientes grandes de otros, o al revés. Ries
Centeno considera un ligero predominio en la mujer, respecto al hombre, Wirth da
un porcentaje del 48,4 para el sexo femenino y un 51,5% para el sexo masculino.
porcentaje
de dientes retenidos que la raza negra, ya que en esta última, el desarrollo y
dimensiones de los maxilares son mayores. Se plantea un hecho establecido en
genética que en realidad se hace ley. Un individuo puede heredar los maxilares
pequeños de un progenitor y los dientes grandes de otros, o al revés. Ries
Centeno considera un ligero predominio en la mujer, respecto al hombre, Wirth da
un porcentaje del 48,4 para el sexo femenino y un 51,5% para el sexo masculino.|
Copyright © 2023 Dr.Javier Saldivar V. All Rights Reserved.
|
